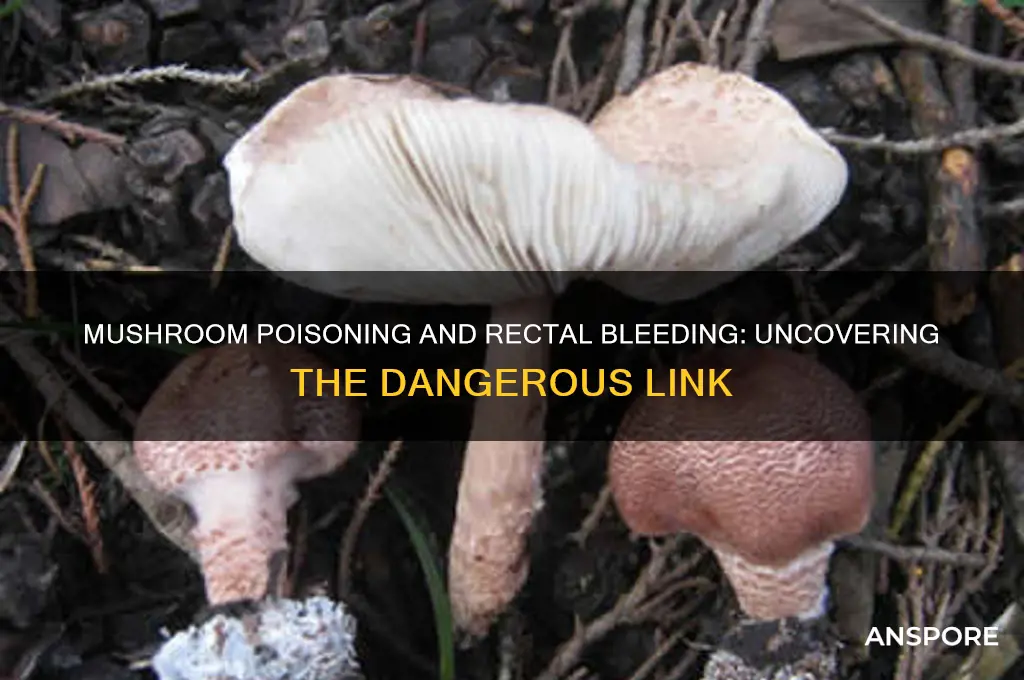
Mushroom poisoning, resulting from the ingestion of toxic fungi, can lead to a range of severe symptoms depending on the species involved. While gastrointestinal distress, such as nausea, vomiting, and diarrhea, is common, more serious cases may involve organ damage or systemic toxicity. Rectal bleeding, though less frequently reported, has been documented in some instances of mushroom poisoning, particularly with certain highly toxic species like Amanita phalloides or Amanita ocreata. This symptom is often associated with severe liver or kidney damage, which can disrupt normal clotting mechanisms or cause gastrointestinal hemorrhage. Prompt medical attention is crucial if rectal bleeding occurs after mushroom ingestion, as it may indicate life-threatening toxicity requiring immediate intervention.
| Characteristics | Values |
|---|---|
| Can mushroom poisoning cause rectal bleeding? | Yes, in some cases. |
| Mushroom species associated with rectal bleeding | Amanita species (e.g., Death Cap, Destroying Angel), Galerina, Lepiota, and some Cortinarius species. |
| Mechanism of rectal bleeding | Toxins like amatoxins and orellanine cause severe gastrointestinal irritation, leading to inflammation, ulceration, and bleeding in the digestive tract, including the rectum. |
| Onset of symptoms | Typically 6–24 hours after ingestion, depending on the toxin. |
| Other symptoms accompanying rectal bleeding | Abdominal pain, nausea, vomiting, diarrhea, dehydration, liver/kidney failure (in severe cases). |
| Severity | Can range from mild to life-threatening, depending on the mushroom species and amount consumed. |
| Treatment | Immediate medical attention, gastric decontamination, supportive care, and in severe cases, liver transplantation. |
| Prevention | Avoid consuming wild mushrooms unless positively identified by an expert. |
| Prognosis | Varies; early treatment improves outcomes, but delayed treatment can lead to organ failure or death. |
Explore related products





What You'll Learn
![]()
Symptoms of Mushroom Poisoning
Mushroom poisoning manifests through a spectrum of symptoms, often dependent on the species ingested and the amount consumed. While gastrointestinal distress—nausea, vomiting, diarrhea, and abdominal pain—is common, more severe cases can involve neurological symptoms like confusion, hallucinations, or seizures. However, the question of whether mushroom poisoning can cause rectal bleeding is less straightforward. Rectal bleeding is not a typical symptom of most mushroom poisonings but has been anecdotally reported in rare, severe cases, particularly with certain toxic species. For instance, the Amanita genus, known for its deadly varieties, can cause gastrointestinal hemorrhage in extreme poisonings, which might include rectal bleeding as a secondary complication.
Analyzing the mechanism, rectal bleeding in mushroom poisoning is likely tied to severe toxin-induced damage to the gastrointestinal tract. Amatoxins, found in Amanita phalloides (Death Cap) and Amanita ocreata (Destroying Angel), cause cellular necrosis in the liver, kidneys, and intestinal lining. This necrosis can lead to bleeding in the digestive tract, potentially extending to the rectum in critical cases. Dosage plays a critical role here—ingesting as little as 30 grams of Amanita phalloides can be fatal for an adult, with symptoms escalating over 6–24 hours. Early intervention, including activated charcoal administration and supportive care, is crucial to mitigate such outcomes.
Instructively, if rectal bleeding is suspected after mushroom ingestion, immediate medical attention is non-negotiable. Do not wait for symptoms to worsen, as delayed treatment increases the risk of organ failure and death. Bring a sample of the mushroom (if safely possible) to aid identification. For prevention, adhere strictly to foraging guidelines: only consume mushrooms positively identified by an expert, avoid wild mushrooms altogether if unsure, and educate children about the dangers of ingesting unknown fungi. Practical tips include cooking all mushrooms thoroughly, as some toxins are heat-sensitive, though this does not apply to amatoxins.
Comparatively, while rectal bleeding is rare in mushroom poisoning, it aligns with symptoms of other toxin-induced gastrointestinal syndromes, such as heavy metal poisoning or certain bacterial infections. The key differentiator is the presence of neurological or hepatic symptoms, which are hallmark indicators of mushroom toxicity. For instance, orellanine poisoning from Cortinarius species causes renal failure without gastrointestinal bleeding, while muscarine poisoning from Clitocybe species induces sweating and salivation without affecting the gut. This specificity underscores the importance of accurate diagnosis and targeted treatment.
Descriptively, the progression of symptoms in severe mushroom poisoning can be harrowing. Initial nausea and vomiting may give way to a deceptive "honeymoon phase" of apparent recovery, lasting 24–72 hours, before severe symptoms like jaundice, seizures, or gastrointestinal bleeding emerge. Rectal bleeding, if present, would likely occur in this late phase, accompanied by shock, organ failure, and potential coma. Survival depends on prompt administration of antidotes like silibinin (for amatoxins) and intensive care support. This grim trajectory highlights why mushroom poisoning demands urgent, informed action—misidentification can turn a meal into a medical emergency.
Growing Porcini Mushrooms in Utah: Tips and Feasibility Guide
You may want to see also
![]()
Types of Toxic Mushrooms
Mushroom poisoning can indeed cause rectal bleeding, though this symptom is relatively rare and typically associated with specific toxic species. Among the thousands of mushroom varieties, only a handful are known to produce severe gastrointestinal distress, including bleeding. The Amanita genus, particularly *Amanita phalloides* (Death Cap) and *Amanita ocreata* (Destroying Angel), contains amatoxins that can lead to liver failure, gastrointestinal hemorrhage, and, in severe cases, rectal bleeding. These toxins are not neutralized by cooking and can cause symptoms within 6–24 hours of ingestion. Immediate medical attention is critical, as delayed treatment significantly increases the risk of fatality.
Not all toxic mushrooms operate through amatoxins. *Clitocybe dealbata* (Ivory Funnel) and *Clitocybe rivulosa* (False Champignon) contain muscarine, a toxin that primarily affects the nervous system but can also cause severe gastrointestinal symptoms, including bleeding. Unlike amatoxin poisoning, muscarine symptoms appear rapidly, often within 15–30 minutes of ingestion. These mushrooms are often misidentified as edible species due to their unassuming appearance, making proper identification crucial. A single cap of *Clitocybe dealbata* can contain enough muscarine to induce symptoms in an adult, though fatalities are rare.
Another category of toxic mushrooms includes those containing orellanine, such as *Cortinarius rubellus* (Deadly Webcap) and *Cortinarius orellanus* (Fool’s Webcap). Orellanine causes delayed renal failure, but gastrointestinal symptoms, including rectal bleeding, can occur in the early stages. These mushrooms are particularly dangerous because symptoms may not appear for 2–3 days after ingestion, leading to delayed treatment. Even small amounts—as little as 10–20 grams—can cause severe toxicity. Foraging without expertise in these species is highly discouraged, as they often grow in similar habitats to edible mushrooms.
Preventing mushroom poisoning begins with accurate identification. Never consume wild mushrooms unless you are absolutely certain of their species, and avoid foraging without an experienced guide. If poisoning is suspected, immediately contact a poison control center or seek emergency medical care. Bring a sample of the mushroom for identification, as this can expedite treatment. While rectal bleeding is not a common symptom of mushroom poisoning, its presence indicates severe toxicity and requires urgent intervention. Awareness of these toxic species and their effects can save lives and reduce the risk of misidentification.
Breathing Magic Mushroom Spores: Can It Induce a Psychedelic High?
You may want to see also
![]()
Gastrointestinal Effects of Toxins
Mushroom poisoning can indeed lead to rectal bleeding, but this symptom is not universal across all toxic species. The gastrointestinal effects of mushroom toxins vary widely depending on the type of mushroom ingested and the specific toxins involved. For instance, amatoxins found in *Amanita phalloides* (Death Cap) and *Amanita ocreata* (Destroying Angel) cause severe liver damage, but initial symptoms often include violent gastrointestinal distress—abdominal pain, diarrhea, and vomiting—without rectal bleeding. In contrast, orellanine-containing mushrooms like *Cortinarius rubellus* and *Cortinarius orellanus* primarily target the kidneys, leading to renal failure, though gastrointestinal symptoms like nausea and vomiting may precede this. Rectal bleeding is more commonly associated with mushrooms containing hemolytic toxins, such as those in *Clitocybe acromelalga*, which can cause gastrointestinal irritation severe enough to lead to blood in the stool.
Understanding the mechanism of toxin action is crucial for recognizing and treating mushroom poisoning. Amatoxins, for example, inhibit RNA polymerase II, disrupting protein synthesis in cells, particularly in the liver and gastrointestinal tract. This results in rapid cell death, leading to symptoms like diarrhea and vomiting within 6–24 hours of ingestion. Orellanine, on the other hand, causes tubular necrosis in the kidneys, but its initial gastrointestinal effects are milder and often overlooked. Hemolytic toxins directly damage red blood cells, leading to hemolysis and potential gastrointestinal bleeding, including rectal bleeding, in severe cases. Dosage plays a critical role; even small amounts of amatoxins (as little as 0.1 mg/kg body weight) can be fatal, while larger quantities of less potent toxins may be required to cause significant harm.
When assessing gastrointestinal symptoms in suspected mushroom poisoning, it’s essential to differentiate between toxin types and their onset times. Amatoxin poisoning typically presents with a biphasic pattern: initial gastrointestinal symptoms subside after 24 hours, followed by a more severe phase of liver failure 48–72 hours post-ingestion. Orellanine poisoning shows a slower progression, with gastrointestinal symptoms appearing within 3–24 hours, followed by renal failure days later. Hemolytic toxin poisoning may cause immediate and persistent gastrointestinal irritation, including rectal bleeding, within hours of ingestion. Age and health status influence symptom severity; children and the elderly are more susceptible to rapid dehydration from vomiting and diarrhea, while those with pre-existing liver or kidney conditions face higher risks of organ failure.
Practical steps for managing gastrointestinal effects of mushroom toxins include immediate medical intervention and supportive care. Activated charcoal may be administered within 1–2 hours of ingestion to reduce toxin absorption, but its effectiveness diminishes rapidly. Intravenous fluids are critical to prevent dehydration, especially in cases of severe vomiting and diarrhea. For amatoxin poisoning, N-acetylcysteine and silibinin are used to protect liver function, while orellanine poisoning requires aggressive hydration and renal support. In cases of suspected hemolytic toxin ingestion, blood transfusions may be necessary if rectal bleeding or hemolysis is severe. Always seek expert identification of the mushroom species involved, as this guides treatment and prognosis.
In conclusion, while rectal bleeding is a possible but not common symptom of mushroom poisoning, it is most likely associated with hemolytic toxins. The gastrointestinal effects of mushroom toxins depend on the specific toxin, dosage, and individual factors. Prompt recognition of symptoms, accurate identification of the mushroom species, and targeted medical intervention are critical for managing these effects and preventing long-term damage or fatality. Always err on the side of caution and consult a poison control center or healthcare provider immediately if mushroom poisoning is suspected.
Can Store-Bought Mushrooms Be Eaten Raw? Safety Tips Revealed
You may want to see also
Explore related products






![]()
Rectal Bleeding Causes and Links
Rectal bleeding, though alarming, can stem from a variety of causes, ranging from benign to severe. One lesser-known but critical trigger is mushroom poisoning. Certain mushrooms contain toxins that irritate the gastrointestinal tract, leading to symptoms like diarrhea, vomiting, and, in severe cases, rectal bleeding. For instance, the Amanita genus, particularly *Amanita phalloides* (Death Cap) and *Amanita ocreata* (Destroying Angel), contains amatoxins that cause liver and kidney damage, often accompanied by gastrointestinal distress. If you suspect mushroom poisoning, immediate medical attention is crucial, as delayed treatment can be fatal.
Analyzing the link between mushroom poisoning and rectal bleeding reveals a dose-dependent relationship. Amatoxins, for example, are harmful even in small quantities—ingesting as little as 50 grams of *Amanita phalloides* can be lethal for an adult. The severity of symptoms, including rectal bleeding, correlates with the amount consumed and the time elapsed before treatment. Other toxic mushrooms, like *Clitocybe dealbata* (Ivory Funnel), contain muscarine, which causes gastrointestinal irritation but is less likely to induce rectal bleeding unless consumed in large amounts. Always avoid wild mushrooms unless identified by a mycologist, as misidentification is a common cause of poisoning.
From a practical standpoint, recognizing the signs of mushroom poisoning is essential for timely intervention. Early symptoms include nausea, abdominal pain, and diarrhea, which may progress to dehydration and, in severe cases, rectal bleeding. If exposure is suspected, induce vomiting only if advised by poison control, as it can worsen certain types of poisoning. Instead, preserve a sample of the mushroom for identification and seek emergency care immediately. Treatment may include activated charcoal, intravenous fluids, and, in extreme cases, liver transplantation for amatoxin poisoning.
Comparatively, rectal bleeding from mushroom poisoning differs from other causes, such as hemorrhoids or inflammatory bowel disease, in its acute onset and association with other systemic symptoms. Hemorrhoids typically cause painless bleeding during bowel movements, while inflammatory bowel disease presents with chronic symptoms like weight loss and fatigue. Mushroom poisoning, however, is marked by rapid deterioration, often within 6–24 hours of ingestion. This distinction underscores the importance of a detailed medical history, including recent dietary exposures, when evaluating rectal bleeding.
In conclusion, while rectal bleeding is a rare symptom of mushroom poisoning, it serves as a red flag for severe toxicity. Awareness of toxic mushroom species, prompt recognition of symptoms, and immediate medical intervention are critical to preventing life-threatening complications. Always exercise caution when foraging wild mushrooms, and when in doubt, err on the side of safety by avoiding consumption altogether. Understanding the unique causes and links of rectal bleeding in this context can save lives and reduce the risk of misdiagnosis.
Can Dogs Safely Eat Mushroom Pate? A Pet Owner's Guide
You may want to see also
![]()
Treatment and Medical Intervention
Mushroom poisoning can indeed cause rectal bleeding, though it is a less common symptom compared to gastrointestinal distress, organ failure, or neurological effects. The severity depends on the mushroom species ingested, with toxic varieties like Amanita phalloides (death cap) or Amanita ocreata posing the highest risk. Rectal bleeding in such cases often stems from hepatotoxicity, where liver damage leads to impaired coagulation and subsequent gastrointestinal hemorrhage. Immediate medical intervention is critical to prevent life-threatening complications.
Upon suspicion of mushroom poisoning, the first step is to contact a poison control center or seek emergency medical care. Activated charcoal may be administered within the first hour post-ingestion to limit toxin absorption, though its efficacy diminishes rapidly. For severe cases, particularly those involving Amanita species, intravenous silibinin (a milk thistle derivative) is used to protect liver cells. Dosage typically ranges from 20–40 mg/kg/day, administered via continuous infusion. Supportive care, including fluid resuscitation and electrolyte management, is essential to stabilize the patient while the body attempts to eliminate toxins.
In cases where rectal bleeding occurs, medical professionals prioritize hemodynamic stability and coagulation support. Blood transfusions may be necessary if bleeding is significant, while vitamin K administration can help reverse coagulopathy caused by liver dysfunction. For patients with acute liver failure, N-acetylcysteine (NAC) is often given to mitigate hepatotoxic effects, with dosages tailored to weight and severity. Continuous monitoring of liver enzymes, prothrombin time, and hemoglobin levels is crucial to guide treatment adjustments.
Prevention remains the most effective strategy. Avoid consuming wild mushrooms unless identified by a mycologist. Educate children and adults about the dangers of foraging without expertise. If exposure occurs, preserve a sample of the mushroom for identification, as this aids in determining the appropriate treatment. Time is of the essence; delays in seeking care can exacerbate symptoms, including rectal bleeding, and increase the risk of irreversible damage. Prompt action and informed medical intervention are key to a favorable outcome.
Mushrooms and Love: Exploring the Emotional Effects of Psilocybin
You may want to see also
Frequently asked questions
Yes, certain toxic mushrooms can cause gastrointestinal symptoms, including rectal bleeding, due to irritation or damage to the digestive tract.
Mushrooms containing toxins like amatoxins (e.g., *Amanita phalloides*) or orellanine (e.g., *Cortinarius* species) can lead to severe gastrointestinal distress, including rectal bleeding, as part of their poisoning symptoms.
Symptoms like rectal bleeding typically appear within 6 to 24 hours after ingestion, depending on the type of mushroom and the toxins involved. Immediate medical attention is crucial if poisoning is suspected.































